Stuart and I met with Dr. Hellner for about an hour this morning and discussed my history, her initial thoughts (lymphoma) and possible next steps. She explained to us that there are two main types of lymphoma, Hodgkin's Lymphoma (HL) and Non-Hodgkin's Lymphoma (NHL). She mentioned that at my age (36), I was certainly in the age group for Hodgkin's Lymphoma, although Non-Hodgkin's Lymphoma was certainly a possibility as well.
For all the nerds in the group, Hodgkin's has a bi-modal distribution, meaning that it is most common (modal) at two (bi-) points in life. It is most likely to be diagnosed in people in their twenties or thirties. It is less common in middle age and becomes more common again after age 60. Non-Hodgkin's occur more often as your age increases. The cause of Lymphoma is unknown, the prognosis varies based on type and stage, but inevitably the treatment is some type of chemotherapy.
Here are the websites that I have visited and would like to share.
Lymphoma Research Foundation http://www.lympoma.org/
The Leukemia & Lymphoma Society http://www.leukemia-lymphoma.org/
National Cancer Institute http://www.cancer.gov/
American Cancer Society http://www.cancer.org/
Both Stuart and I left Dr. Hellner's office glad that we went. We both had a sense of realism that having cancer would not be ideal, but that Lymphoma is curable.
Next steps are to go forward with the mediastinoscopy tomorrow morning to try to get more biopsy tissue, as well as to schedule appointments next week for heart and lung tests (baselines prior to chemotherapy).
On a lighter note, my Mom came down this evening and will be staying with us through Sunday to help with the kids and the house.
Thursday, September 30, 2010
Wednesday, September 29, 2010
29th - Good news is bad news
Dr. Reames called this afternoon to tell me that the pathology department called and the tissue from Monday's bronchoscopy was "non-diagnostic". Technically, it means that there were no malignant cells found, which I took as good news. Those in the medical profession took it as a disappointment however, as they do not seem to want to call it quits without an adequate explanation for the golf ball sized lymph nodes in my chest. Go figure.
At this point, I think everyone but me believes that I have Lymphoma. My resolve has started to give way, so I decided it was time to see that Oncologist for a consultation.
Dr. Kersten recommended Mariealane B. Hellner, MD, who practices near my house and is supposed to be very good. Stuart and I will go to her office in the morning.
At this point, I think everyone but me believes that I have Lymphoma. My resolve has started to give way, so I decided it was time to see that Oncologist for a consultation.
Dr. Kersten recommended Mariealane B. Hellner, MD, who practices near my house and is supposed to be very good. Stuart and I will go to her office in the morning.
Tuesday, September 28, 2010
28th - A second biospsy
Dr. Davis knew the bronchoscopy might not get enough tissue to provide a definitive diagnosis, so she referred me to Mark K. Reames Sr., MD, FACS, who could perform a mediastinoscopy to get a better tissue sample if necessary. Mediastinoscopy is a surgery that allows doctors to view the middle of the chest cavity and to do minor surgery through very small incisions. It allows surgeons or pulmonary doctors to remove lymph nodes from between the lungs and to test them for cancer or infection.
Dr. Reames is the classic southern gentleman and I felt comfortable with him from the start. Although I was anxious to get going and get to a diagnosis, he counseled me that having a procedure before the full pathology was back on from the bronchoscopy might be rash.
We spoke for a short while and then parted ways. I was hoping that someone would call me and tell me this whole thing was a joke, but the reality was that I would see the fine Dr. Reames on Friday.
Dr. Reames is the classic southern gentleman and I felt comfortable with him from the start. Although I was anxious to get going and get to a diagnosis, he counseled me that having a procedure before the full pathology was back on from the bronchoscopy might be rash.
We spoke for a short while and then parted ways. I was hoping that someone would call me and tell me this whole thing was a joke, but the reality was that I would see the fine Dr. Reames on Friday.
Monday, September 27, 2010
27th - Surgeons & rock music
Special thanks today to our fantastic neighbor, Bridget Ruller, who came to our house at the crack of dawn to help with our 2 children (our daughter Peyton - 5 and our son Cooper - 3).
Stuart and I drove to Carolinas Medical Center at 6:30 AM for an 8 AM bronchoscopy with Dr. Davis and Jaspal Singh, MD, MHA. Dr. Singh is a very good surgeon, has a decent sense of humor and loves to work while listening to classic rock music.
The procedure itself was not bad at all from my point of view. It is done under mild to moderate sedation, which makes sense when someone is going to put a tube, camera and instrument set down your throat. Dr. Davis mentioned prior to the procedure that the sedative worked on the same receptors as red wine, which is another of my true loves. Suffice it to say that they used all the sedative they had on hand and still had to wrap up early when I started to wake up and 'get involved'. They did accomplish the point of the procedure however, which was to obtain some tissue from one of my lymph nodes to send for biopsy.

A picture of a surgeon (certainly not Dr. Singh) performing a bronchoscopy (that is not my nose).
Stuart and I drove to Carolinas Medical Center at 6:30 AM for an 8 AM bronchoscopy with Dr. Davis and Jaspal Singh, MD, MHA. Dr. Singh is a very good surgeon, has a decent sense of humor and loves to work while listening to classic rock music.
The procedure itself was not bad at all from my point of view. It is done under mild to moderate sedation, which makes sense when someone is going to put a tube, camera and instrument set down your throat. Dr. Davis mentioned prior to the procedure that the sedative worked on the same receptors as red wine, which is another of my true loves. Suffice it to say that they used all the sedative they had on hand and still had to wrap up early when I started to wake up and 'get involved'. They did accomplish the point of the procedure however, which was to obtain some tissue from one of my lymph nodes to send for biopsy.

A picture of a surgeon (certainly not Dr. Singh) performing a bronchoscopy (that is not my nose).
Friday, September 24, 2010
24th - Time for a biopsy
I went into see Dr. Kersten this morning for the formal report out of the CT results. Dr. Kersten walked my wife (Stuart) and me through the report and images, then told us that the next step was a biopsy, then a consultation with someone in Oncology (cancer doctor).
Later in the afternoon, we saw a pulmonologist named Juhayna K. Davis, MD for a consultation on the options available to obtain tissue for the biopsy. Dr. Davis was fantastic, despite the fact that I told her she needed to have the picture on her website changed for the better. I simply suggested that someone on the list of Charlotte's Top Doctors 2010 should have a glamour shot. Back to the point, Dr. Davis recommended that I opt for a less invasive procedure first. This procedure, called a bronchoscopy, is scheduled for 8 AM Monday morning.
Later in the afternoon, we saw a pulmonologist named Juhayna K. Davis, MD for a consultation on the options available to obtain tissue for the biopsy. Dr. Davis was fantastic, despite the fact that I told her she needed to have the picture on her website changed for the better. I simply suggested that someone on the list of Charlotte's Top Doctors 2010 should have a glamour shot. Back to the point, Dr. Davis recommended that I opt for a less invasive procedure first. This procedure, called a bronchoscopy, is scheduled for 8 AM Monday morning.
Thursday, September 23, 2010
23rd - Abnormal soft tissue
Dr. Kersten called me around lunchtime to tell me that I needed to come back in as soon as possible to see him and have a CT scan of my chest done. The radiologist that read my X-ray after Dr. Kersten noted some abnormal soft tissue in my right paratracheal region.
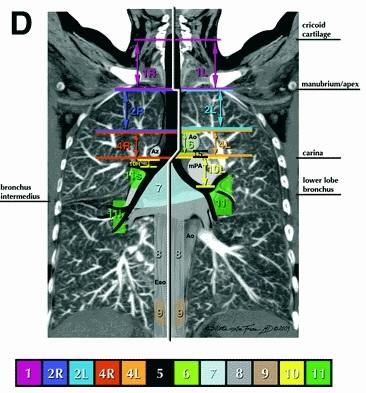
The CT scan took about 30 minutes and the results were ready right away. The CT scan showed significant lymphadenopathy (a.k.d. disease of the lymph nodes) in the right paratracheal space and the right anterior prevascular space. There were also mildly enlarged low right cervical/supraclavicular lymph nodes present and mild precarinal lymphadenopathy. For those medically inclined, I have included a couple lymph node maps below (these are not images of me!!!). For those not so inclined, suffice it to say a had a lot of enlarged lymph nodes on the right side of my lower neck and center of my chest...with the largest two the size of a golf ball (which is at least 1.680 inches or 42.67 millimeters in diameter for you trivia nuts). These results were suggestive of lymphoma, but again, I was in denial.
 Frontal view of Figure-D shows right paratracheal (2R and 4R) and low right cervical/supraclavicular (1) lypmh node spaces. Diagram by Annie Frazier, MD.
Frontal view of Figure-D shows right paratracheal (2R and 4R) and low right cervical/supraclavicular (1) lypmh node spaces. Diagram by Annie Frazier, MD.
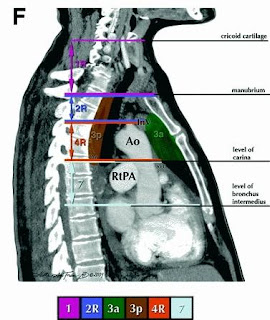 Sagittal view of Figure-F shows right prevascular (3a) and precarinal lymph node spaces. Diagram by Annie Frazier, MD.
Sagittal view of Figure-F shows right prevascular (3a) and precarinal lymph node spaces. Diagram by Annie Frazier, MD.
The CT scan took about 30 minutes and the results were ready right away. The CT scan showed significant lymphadenopathy (a.k.d. disease of the lymph nodes) in the right paratracheal space and the right anterior prevascular space. There were also mildly enlarged low right cervical/supraclavicular lymph nodes present and mild precarinal lymphadenopathy. For those medically inclined, I have included a couple lymph node maps below (these are not images of me!!!). For those not so inclined, suffice it to say a had a lot of enlarged lymph nodes on the right side of my lower neck and center of my chest...with the largest two the size of a golf ball (which is at least 1.680 inches or 42.67 millimeters in diameter for you trivia nuts). These results were suggestive of lymphoma, but again, I was in denial.

Wednesday, September 22, 2010
22nd - Did I inhale?
My story started on a Wednesday afternoon, with a normal trip to the doctor's office. As with many of you, I do not have a "primary care doctor" in the traditional sense, I usually just take my chances with whomever is available when I need to be seen. Luckily for me in this case, I drew a wonderfully thorough gentleman, Brian P. Kersten, MD. My chief complaint was a delicate matter and not very relevant to you, so I will leave it out. As a secondary issue, I complained to Dr. Kersten of some chest tightness that had been bothering me for a couple weeks. My hope was that the worst thing that it could be was a bad effect from my recent trip to Prague, CZ, where I rode in the front seat of an antique Praga Alfa car and inhaled fumes for hours during a tour. Dr. Kersten ordered an EKG and an X-ray of my chest, which initially showed nothing noteworthy.

The pre-1940 Praga Alpha
The pre-1940 Praga Alpha
22nd - Two weeks of Hell
You may find it more than a little funny that I am sitting in front of my computer starting a blog. If you know me well, the reasons are obvious and many; if you do not know me that well or we have been out of touch for a while, suffice it to say that I have made endless fun of bloggers over the past few years. As with most (modestly) insecure people, I tend to make fun of things that I am afraid of, jealous of, or in general do not think I would be very good at. So, for me, blogging ranks up there with hermit crabs (I refuse to touch them), celebrities (both a fear and jealousy depending on who we are talking about), and speaking foreign languages (I need to pick a few up).
The reason for this blog is efficiency, something I have a particular love affair with. Without the blog, I know that I will not do a good job keeping all the people I should up to speed on my new challenge. The challenge is this...to overcome Hodgkin's Lymphoma, which I will be formally diagnosed with in two weeks time, on 6 October, 2010. You will hear all about Hodgkin's through this blog, so I will spare you the details in this post. In short, Hodgkin's is a form of cancer that affects the lymphatic system, which is part of the immune system.
Now that I have shared my diagnosis with you, I will fill you in on all the events leading up to the diagnosis. It turns out to be exactly two weeks of Hell between my first doctor's appointment and my diagnosis. My state of mind was pure denial the entire time.
The reason for this blog is efficiency, something I have a particular love affair with. Without the blog, I know that I will not do a good job keeping all the people I should up to speed on my new challenge. The challenge is this...to overcome Hodgkin's Lymphoma, which I will be formally diagnosed with in two weeks time, on 6 October, 2010. You will hear all about Hodgkin's through this blog, so I will spare you the details in this post. In short, Hodgkin's is a form of cancer that affects the lymphatic system, which is part of the immune system.
Now that I have shared my diagnosis with you, I will fill you in on all the events leading up to the diagnosis. It turns out to be exactly two weeks of Hell between my first doctor's appointment and my diagnosis. My state of mind was pure denial the entire time.
Subscribe to:
Posts (Atom)